Session Three — Pediatric Endoscopy (CHONY)
At the The Laura Rothenberg Bronchoscopy and Endoscopy Center. Doctor is a specialist in short bowel syndrome. Joined by a Pediatric GI fellow.
Endoscopy Information Management
Software used was ProVation MD, a specialized GI tool. It looks like this. They used it side-by-side with EPIC. There was some synergy between the tools apropos data-sharing but much left to be desired. For billing you imported from provation to EPIC. Same for medication reconciliation. Pronounced, frustrating lag between systems.
They first populated a tree by adding nodes to it (right-click, select type) which would then populate the note on the right hand panel. CPT codes were added manually from memory or via search (small, tenable grumbling about this state of affairs.) Endoscope name and model put into this tree: ascertained several times; fellow took a picture for later (“What was the scope?”)
Photos taken during endoscopy were annotated with numbers and each number was associated with a region on an image that looked like this.
Patients
Patient I
~10 yo F. Duodenal polyops. No polypectomy performed; deemed unnecessary by another physician (“First, do no harm”).
GLP-2 can cause polyps but this has only ever been reported in adults. This is the first Pediatric case. Paper will be written.
Patient II
~15 yo M. Non-verbal autistic. Endoscopy and Colonoscopy performed. Severe liver cirrhosis (caused by complications from TPN-IV nutrition; kept him alive as a baby but causes complications) → portal hypertension (portal hypertensive gastropathy; high blood pressure in the portal vein) → esophageal varices. Hepatologist was called (“Do No Harm”) to consult over whether the varices should be banded (she and fellow performed procedure on 3-4).
Colonoscopy was complicated and took a long time because of the scope getting coiled and not being able to go past the sigmoid colon. Enlargement was another issue. Colonoscopy completed after a long while. The Colon is Kinky and Complicated.
We also saw the other end of this as a “bubble” during endoscopy (this was the feeding tube). Fellow mentioned that popping this balloon/bubble by mistake would make the tube fall out.
Patient III
~15 yo F. CC: Intestinal discomfort. Produces antibodies to gluten. Blood when wiping. Endoscopy and Colonoscopy performed; took much less time than Patient II. Doctor told me this is typically how things go.
This one ended up having celiac disease.
Random Notes
- Gattex is a GLP-2 agonist (GLP-1 is the thing in the news). It’s “a kind of hormone replacement therapy”. It’s a growth hormone. Prescribed for short bowel syndrome; helps absorb IV nutrition. Can cause polyps. This is normally, natually produced but some kids need it.
- Atresia → Common term for blockage.
- Doctors do not record video (“Unnecessary and I don’t even know how to”); only take pictures.
- Standard procedure: Esophagus → Stomach → Opening of Duodenum → Retroflex (reverse the endoscope; you can see it with it!)
- What happens if a doctor is unavailable physically for a consult? No ‘live-streaming’. They use their iPhones and take pictures or use FaceTime to ‘phone a friend’.
- Opportunity: Is it even possible to use image algos/ML to guide the endoscopist?
- Opportunity: Used Google Images to confirm varices grading.
- Can we use an image algo for this?
- Is there some local MedPedia? Can we do something to capture this knowledge even within NYP?
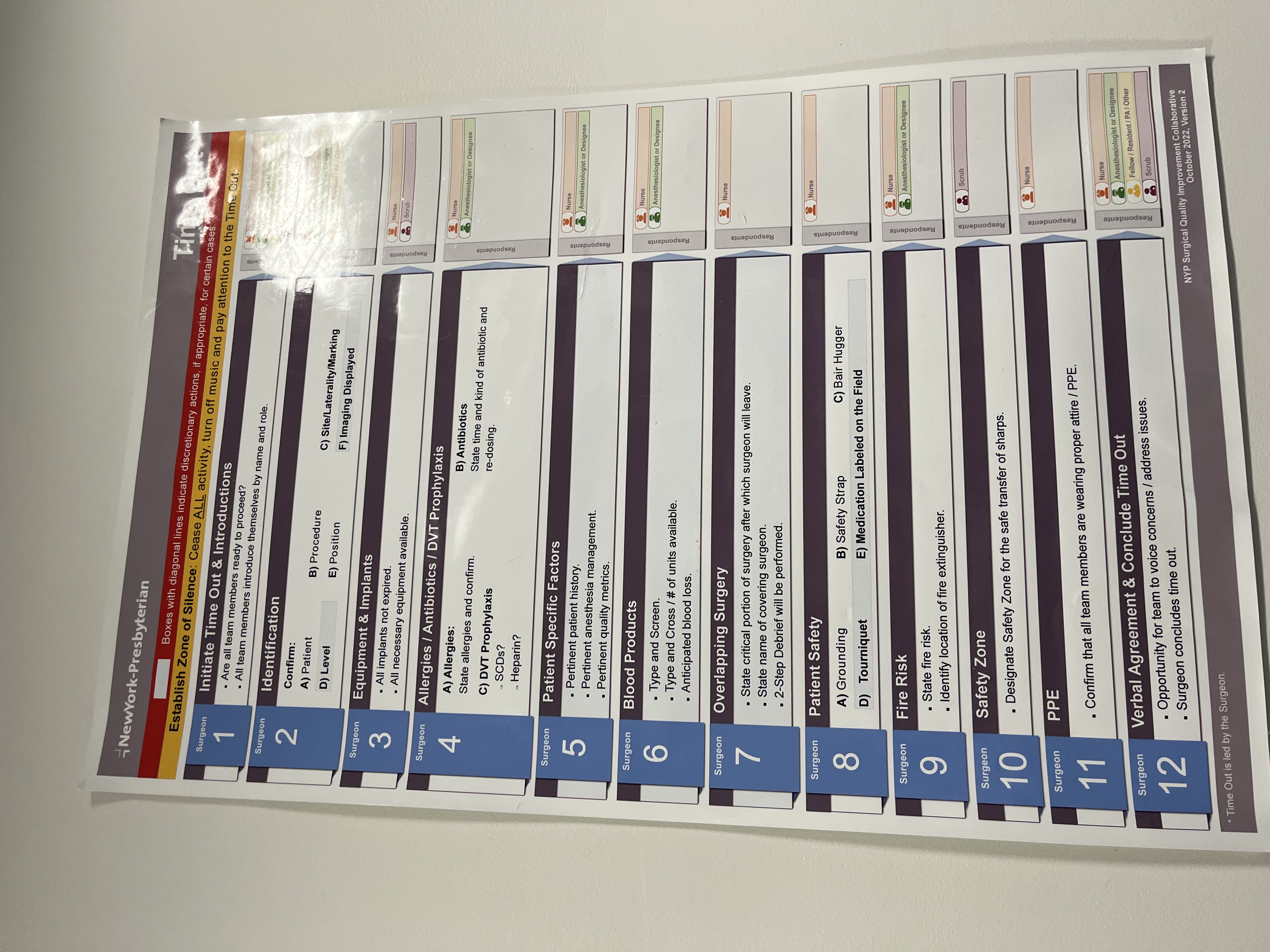
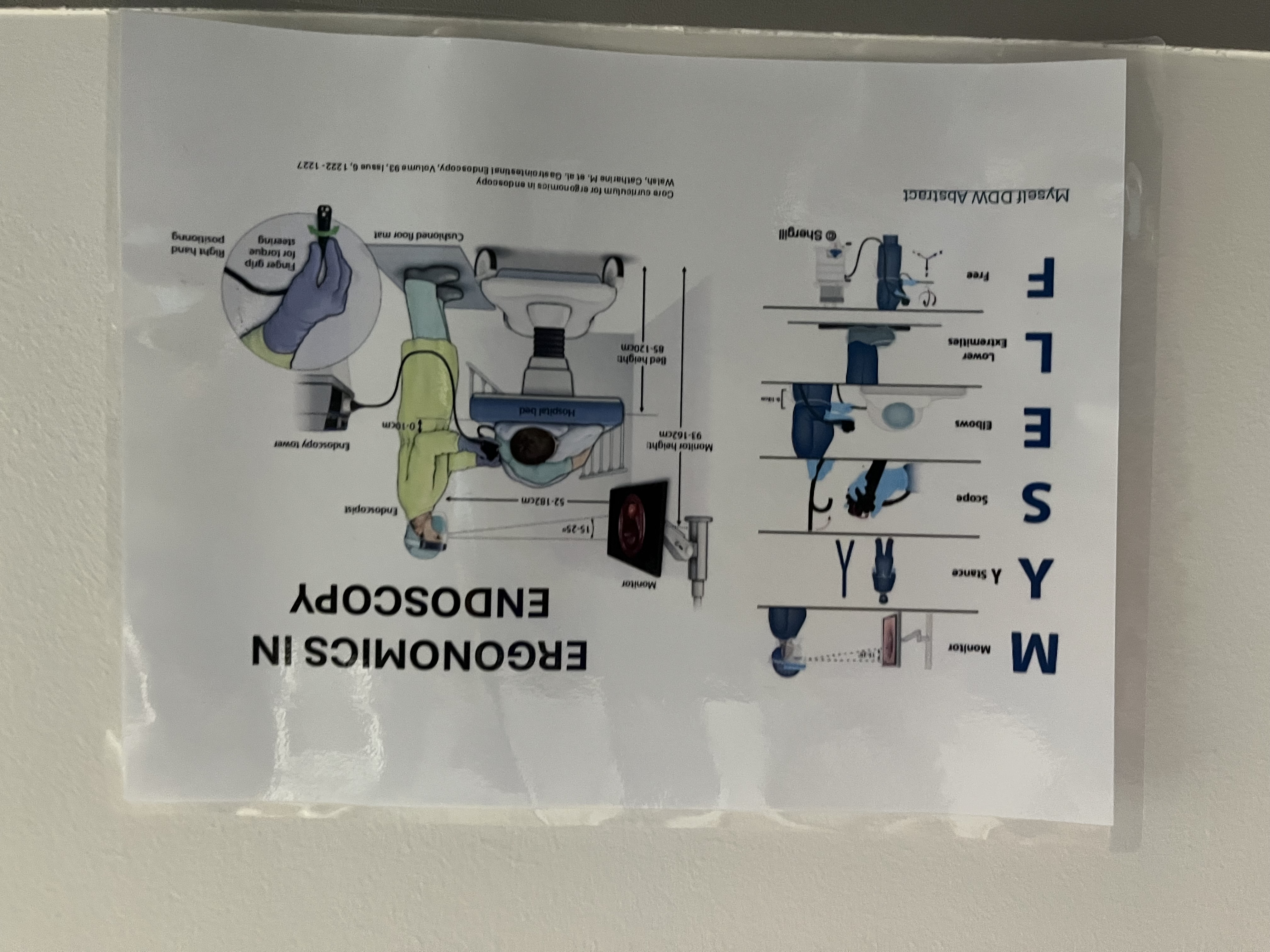
Signs on Walls
The first is a checklist whose text is way too small to be seen from where people are standing! The second appears to be ‘mere guidelines’.