Clinical Nutrition
Notes from a talk by Muying Li, PhD, RD
Registered Dietitian (RD/RDN)
Board certified professionals. Meet the CDR’s criteria to earn the cred. Highly regulated with training requirements and clinical rotations. You are an expert in identifying and treating ddisease-related malnutirition and conducting medical nutrition therapy. Renew every 5 years. Takes minimum ~1,000 hours. You also need a masters degree. You need “CPEU”s — kinda like credits (for every paper, research, conference, poster you have). You need 75 every 5 years. Keeps ya fresh and up to date ya know?
Pass the CDR exam (You are now an RD) → Get Licensure/Certification (You can now practice!)
Guidelines matter only for healthy populations; if you have cancer or other diseases, these change.
Nutritionist has no such requirement! You cannot work in a clinical setting. You can get this shit online. Vibes-based.
Can a Nutritionist call themselves a Dietitian? Can an Astrologer call themselves an Astronomer? Yeah.
You can also become an Advanced RD. You need to be a Board Certified Specialist (e.g. in oncology). There’s also an Advanced Practitioner Certification in Clinical Nutrition (RD-APs).
You can work in Clinic, Research, Education, Government, private practice, Nutrition Supplement companies (lol).
Clinical Nutrition and Why it Matters
Nutrition affects every stage of care: healing (wounds, infections, ulcers), muscle mass, toleration of medical treatment… watch your food! Attitudes around nutrition have changed a lot.
If you are malnourished (i.e. any kind of nutrition imbalance that leads to weight loss, lean body mass loss, loss of fat stores, reduced function), longer stays, higher likelihoods of complicationsa and readmissions, higher costs, higher in-hospital mortalities.
There’s Starvation, Chronic/Disease, and Acute malnutirition (e.g. a gunshot).
People become more malnourished at a hospital! Think about it: you are enfeebled, mentally and physically and subject to nutrient loss, they aren’t handing out cookie dough, you have increased metabolic demand.
Clinical Nutrition is high-impact but not always very visible.
Clinical RD Role
- Tailor nutrition
- Transition of care: education
There are all sorts of Clinical RDs (in/out patient, adult/pediatrics, long-term care, unit (general, oncology, cardiac rehab, renal, etc)/float (a generalist)-based.)
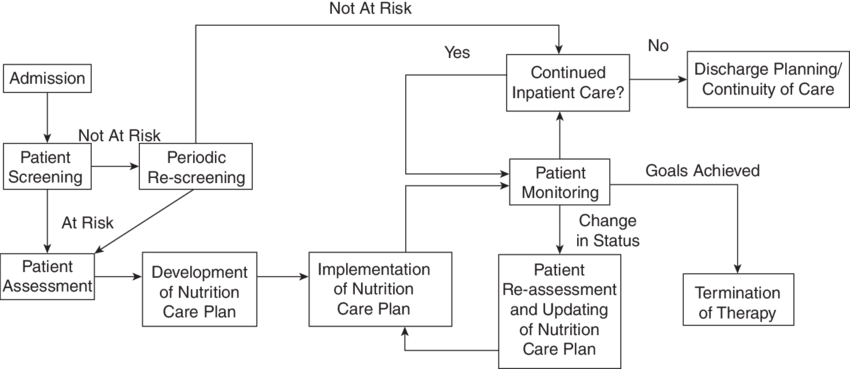
In-Patient Workflow
Home -> Hospital -> (Discharge) ---------> Home (Follow-up Out-patient visits)
| |
| Nutrition Education
|
Initial assessment, follow-ups
Dietitians and physicians ask different questions.
- Is the nutrition adequate?
- Increased needs for protein? Energy?
- What is the safest route? PO, EN, PPN, TPN
- How will we monitor reponse and complications?
- Any drug-food interactions
- etc etc etc
Artifacts and Models
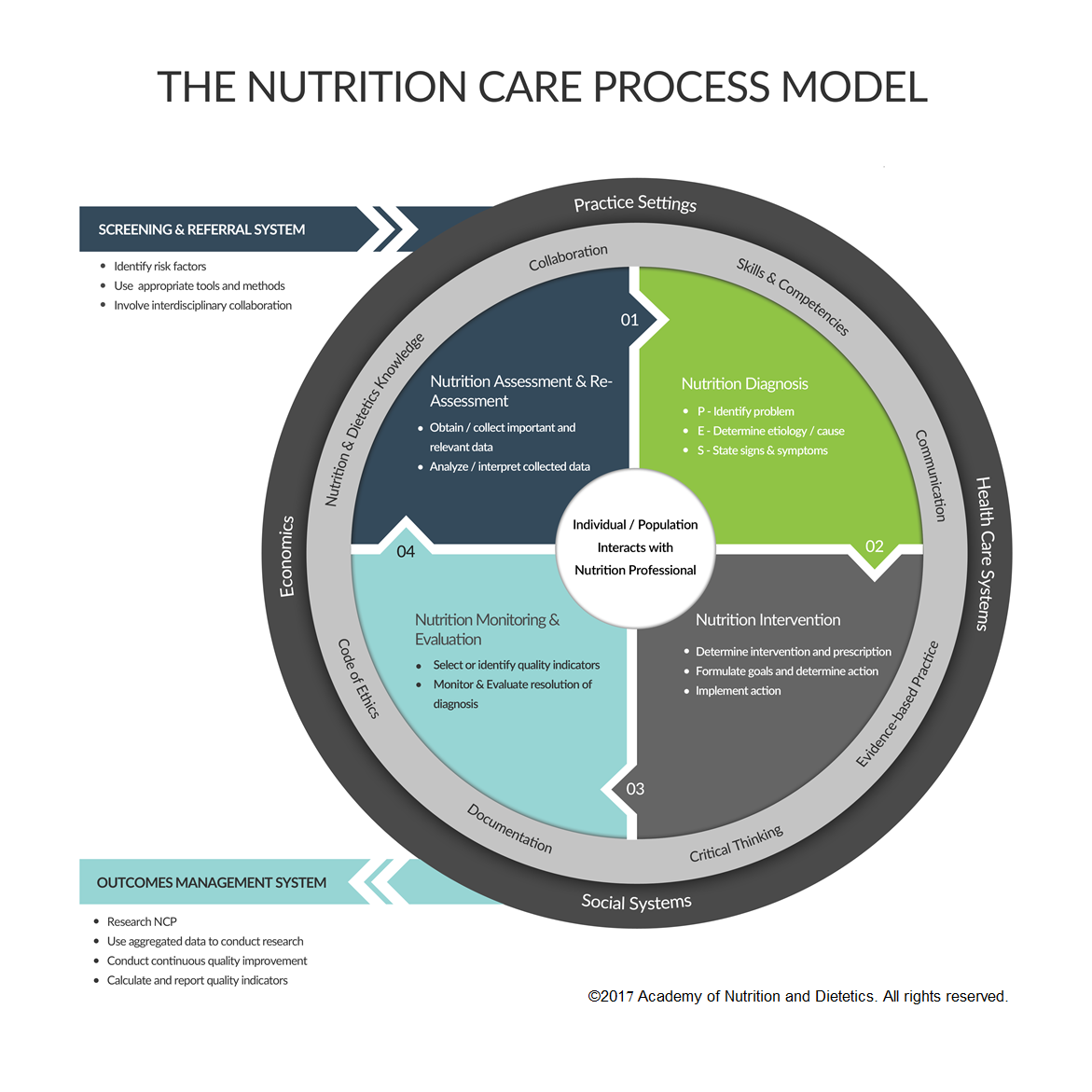
Physicians use SOAP but RDs use ADIME — Assessment, Diagnosis, Interventions, Monitoring, Evaluation.
See also the Nutrition Care Process (NCP) Model.
Basically they look for drugs and conditions that are pertinent to nutrition.
E.g. Propofol: rapid, intravenous sedative-hypnotic. Provides 1.1 kCal/Ml. Now if you take 25 mL/Hr of it you get calories in the day! This is the kind of thing Dietitians think about!
Other things of interest might be Omeprazole (proton-pump inhibitor), MiraLAX (stool softener) or Senokot (stimulates muscle) — they watch for dehydration.
Nutrition Support
Lots of math here. There’s Enteral Nutrition (directly to the gut, AKA Tube Feeding) which is different than Parenteral Nutrition which is through an IV (Central Line).
Note that you really want to have them eat first, tube next, and IV last. If the gut works, use it.
Enteral Nutrition — Short Term: go through nose (easiest), then go through duodenum, and jejunum (through a small hole.)
Enteral Nutrition — Long Term: G-tube (gastronomy tube) or J-tube (jejunostomy tube).
Formulas - provide energy, protein, fluids. Three kinds:
- Polymeric (intact, Ensure, get at CVS)
- Monomeric (pre-digested / hydrolyzed)
- Disease-Specific (DM, CKD, etc)
Nutrition Focused Physical Exam
Edema, Abdomen, Skin, Body Fat Stores, Lean Body Mass Stores (protruding clavicle, there’s less of the Deltoid muscle).
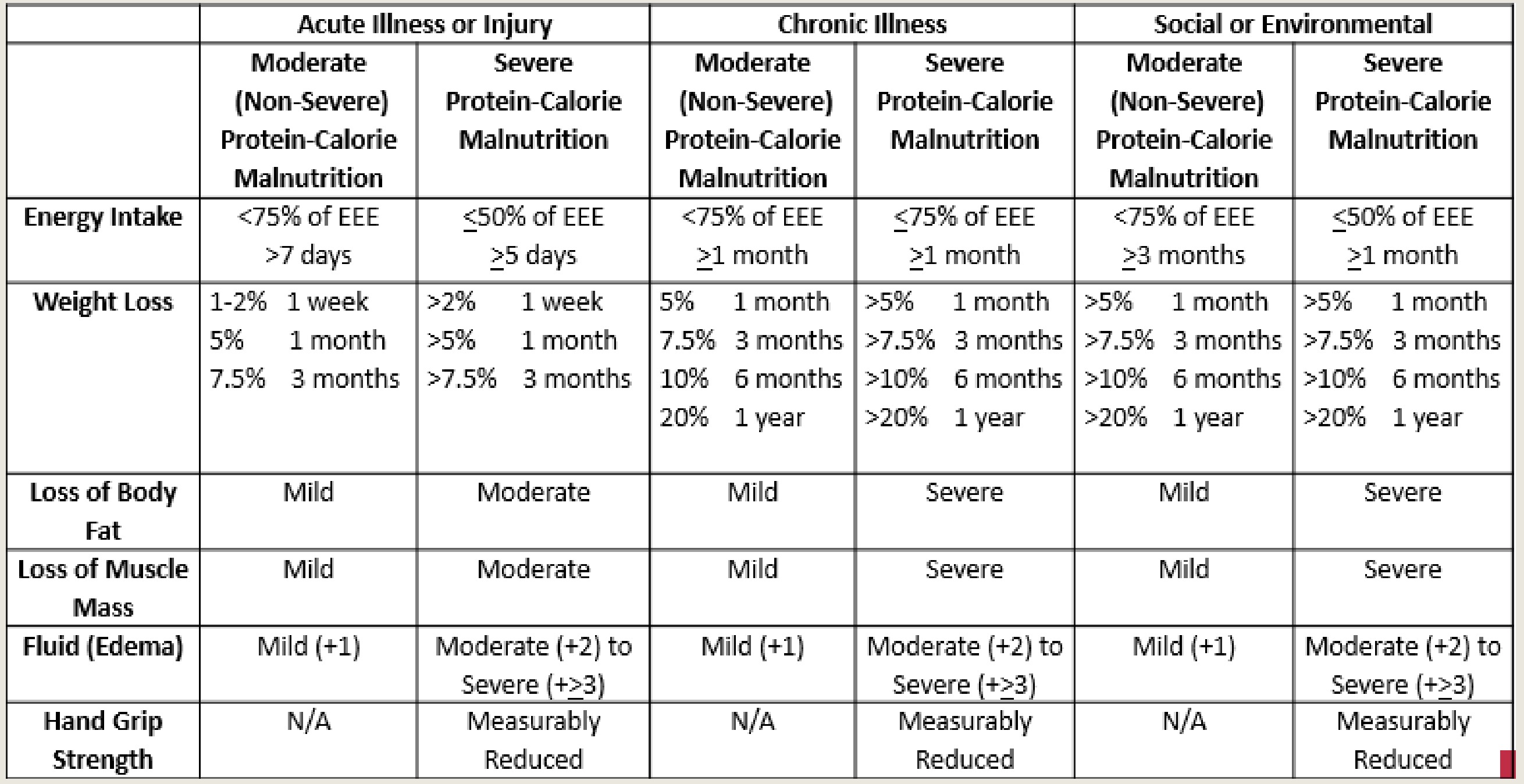
See the ASPEN Criteria that is widely used:
Ideal Body Weight
- Females: 100# for first 5ft, 5# for each additional inch.
- Males: 106# first 5ft, 5# for each additional inch.
BMI is your weight in Kg divided by your height in meters squared. There’s also
Nutrient Needs
Energy
| Patient Type | Estimated Energy Needs |
|---|---|
| Healthy Adult, Ambulatory | 25–30 kcal/kg |
| Healthy Adult, Active | 30–35 kcal/kg |
| Overweight | 21–25 kcal/kg |
| Obese | 18–21 kcal/kg |
| Critically ill, intubated | 25–30 kcal/kg |
| Critically ill (BMI >30) | 11–14 kcal/kg actual body weight |
| Patient Type | Estimated Energy Needs |
|---|---|
| Cancer | 25–35 kcal/kg |
| Cancer, head & neck | 28–32 kcal/kg; 30–40 kcal/kg if wt loss |
| CKD stages 1–4 | 25–30 kcal/kg |
| CKD Stage 5 on dialysis | 30–35 kcal/kg |
| Cirrhosis | 25–35 kcal/kg |
| Transplant, < 6 months post-op | 30–35 kcal/kg |
| Transplant, >6 months post-op | 25–30 kcal/kg |
Protein
| Condition | Protein Requirement |
|---|---|
| DRI Reference | 0.8 g/kg body weight |
| Adult maintenance | 0.8–1 g/kg |
| Older Adults | 1 g/kg |
| Renal disease (pre-dialysis, stage IV) | 0.6–0.8 g/kg |
| Renal disease (hemodialysis) | 1.2–1.3 g/kg (up to 1.5–1.8 g/kg) |
| Hepatitis (acute or chronic) | 1–1.5 g/kg |
| Hepatic encephalopathy | 0.6–0.8 g/kg (BCAA if refractory) |
| Condition | Protein Requirement |
|---|---|
| Organ transplant (short term) | 1.5–2 g/kg |
| Organ transplant (long term) | 1 g/kg |
| Pregnancy | +25 g/day in 2nd & 3rd trimesters |
| Pulmonary disease | 1.2–1.5 g/kg |
| Critical illness (burns, sepsis, TBI) | 1.5–2 g/kg |
| Stroke | 1–1.2 g/kg |
| Condition | Protein Requirement |
|---|---|
| Cancer | 1–1.5 g/kg (1.5–2.5 if cachectic) |
| Bone Marrow Transplant | 1.5 g/kg |
| Inflammatory bowel disease | 1–1.5 g/kg |
| Short bowel syndrome | 1.5–2 g/kg |
| BMI >27, normal renal/liver | 1.5–2 g/kg IBW |
| Obesity Class I or II, trauma (ICU) | 1.9 g/kg IBW |
| Obesity Class III, trauma (ICU) | 2.5 g/kg IBW |
Fluid
Goals
- Maintenance of adequate hydration
- Tissue perfusion
- Electrolyte balance
Needs based on
- Body weight
- Body surface
- RDA
Consider
- Insensible losses: 75% skin, 25% lung (500–900 ml)
- Measured losses: stool (250 ml), urine (800–1500 ml), other drainage
- Fluid balance alterations due to:
- Metabolic changes (fever)
- Disease states (CHF, CKD/dialysis)
- Medical therapy (diuretic treatment)
Factors increasing fluid needs
- Fever: 13% for each 1°C above normal (37°C); ~7% per °F
- Sweating: 10–25%
- Hyperventilation: 10–60%
- Extraordinary wound/fistula, gastric and/or renal fluid losses: varies (based on average 24-hour output)
Based on Age
- Young Adult: 35–40 ml/kg (actual body weight)
- 20–55 years old: 30–35 ml/kg (may be higher if active)
- 55–75 years old: 25–30 ml/kg
-
75 years old: 25 ml/kg; >100 years old: 20 ml/kg
Methods
- RDA Method: 1 ml fluid per 1 kcal of estimated needs
- Fluid Balance Method: Total output + 500 mL/day
Holiday-Segar Method
- < 10 kg: 100 ml/kg
- 11–20 kg: 1000 ml + 50 ml/kg for each kg >10 kg
-
20 kg: 1500 ml + 20 ml/kg for each kg >20 kg
Fluid Requirement Equations
| Method | Details |
|---|---|
| Weight-based (18–55 yr) | 35 mL/kg |
| Weight-based (56–75 yr) | 30 mL/kg |
| Weight-based (>75 yr) | 25 mL/kg |
| Tiered method | 100 mL/kg for 1st 10 kg + 50 mL/kg for 2nd 10 kg + 20 mL/kg (≤50 yr) or +15 mL/kg (>50 yr) |
| Instruction | Take average of the two methods |
| Additional fluids | Add for losses: loose stool, drains, fistulas, ostomy, G-tube output, large draining wounds, emesis, drooling, paracentesis, lactation |
ASPEN Malnutrition Criteria
Severe Malnutrition
| Criteria | Acute Illness | Chronic Illness | Social Circumstances |
|---|---|---|---|
| Weight loss | >2% in 1 wk; >5% in 1 mo; >7.5% in 3 mo | 5% in 1 mo; 7.5% in 3 mo; 10% in 6 mo; 20% in 12 mo | 5% in 1 mo; 7.5% in 3 mo; 10% in 6 mo; 20% in 12 mo |
| Energy intake | ≤50% of needs for 5 d | ≤75% of needs for 1 mo | ≤50% of needs for 1 mo |
| Body fat / muscle | Moderate depletion | Severe depletion | Severe depletion |
| Fluid accumulation | Moderate to severe | Severe | Severe |
| Functional status | Measurably reduced | Measurably reduced | Measurably reduced |
Moderate Malnutrition
| Criteria | Acute Illness | Chronic Illness | Social Circumstances |
|---|---|---|---|
| Weight loss | 1–2% in 1 wk; 5% in 1 mo; 7.5% in 3 mo | 5% in 1 mo; 7.5% in 3 mo; 10% in 6 mo; 20% in 12 mo | 5% in 1 mo; 7.5% in 3 mo; 10% in 6 mo; 20% in 12 mo |
| Energy intake | 75% of needs for 7 d | 75% of needs for 1 mo | 75% of needs for 3 mo |
| Body fat / muscle | Mild depletion | Mild depletion | Mild depletion |
| Fluid accumulation | Mild | Mild | Mild |
| Functional status | Not applicable | Not applicable | Not applicable |
Other
- Nutritional diagnosis Medical diagnosis.
- PES Statement: Problem/Etiology (Root Cause)/Signs+Symptoms — “Inability to eat at this time related to unresponsiveness and mechanical ventilation as evidenced by indication for enteral nutrition support to meet estimated needs.”
Anthropometric Data (Adult)
- Height
- Weight
- BMI (kg/m^2)
- Ideal body weight (IBW)
- Percent ideal body weight
- %IBW = Actual weight / IBW × 100
- Usual body weight (UBW)
- %UBW = Actual weight / UBW × 100
- Percent weight change
- (UBW - Actual Wt) / UBW × 100
IBW
- Females: 100# for first 5 ft + 5# for each additional inch
- Males: 106# for first 5 ft + 6# for each additional inch
- Assumes medium frame size; adjust +/-10% for frame size to estimate an appropriate desirable body weight range
- For height less than 5 ft, subtract 2# for each inch below 5 ft
- Adjusting for amputations
Clinical Nutrition Informatics
Can you name one Clinical Nutrition Informatics tool? Yep. It’s pretty underrepresented.
Why? For one, IV nutrition might be ‘easy’ to capture but oral nutrition is much harder (did they eat things? Did their family bring them food?). Nutrition also changes over time and in context. Information is spread across notes, flowsheets, labs, orders, report. Variables are behavioural, function, social; not just biomedical.
Challenges & Opportunities!
- Poor integration of intake, symptoms, labs, and feeding data
- Weak decision support for consult timing, route selection, and follow-up
- Nutrition problems are often recognized late rather than early
- Earlier identification of nutrition risk
- Better integration of nutrition-relevant data
- Smarter consults and decision support
- Longitudinal monitoring across inpatient and outpatient care
- More personalized and adaptive nutrition interventions
- Better visibility of nutrition within the care team