Health IT and Safety
Medical Errors and Adverse Events overlap. In the latter some are preventable and others not.
See the Betsy Lehman case with cyclophosphamide. A very famous overdose case. 1000 mg/m2 of body surface area but, after reading the trial, the physician prescribed 4,000 mg/m2
See also, poor Lewis Blackman and Josie King. And Willie King, and Jesica Santillan.
Being Honest about Screw-Ups
To err is human.
KEEPSAFE is used for voluntary reporting. The rate is pretty low (“voluntary”). Another tool is the Just Culture Tool. Note that the substitution test here means “If you replaced the person who screwed up with another”.
If you screw up, honesty is the best policy. You don’t need to grovel. “An error was made with your medication.” Most of the time, people understand (and are less likely to sue).
Wrong-patient errors are ~80% caused by interruptions/distractions!
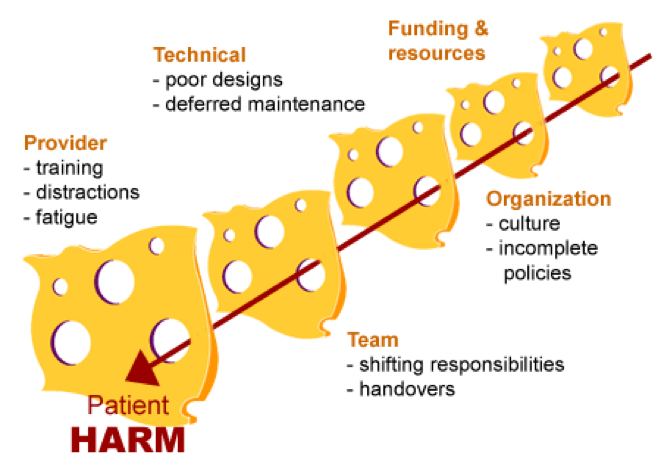
Swiss Cheese Model
Assorted Notes
ID Verify and ID Reentry: the latter had a much higher reduction on reducing errors with patient medications (40% versus 15% DBMI research in 2013). Physicians kinda revolted with these UI intercepts. Pictures help; but think of baby pictures (Jason Adelman: mean number of patients at risk for wrong patient is 50% of average daily census. He (his wife) suggesting adding mom’s name and sex: Catherinesgirl. Kimsboy.)
How many charts do you keep open to avoid errors? Remember that distraction is the #1 reason for patient errors. Two is more of a sweet spot. This depends.
Prof uses pictures to ‘anchor’ on patients. But the pictures can be changed by anyone and will lead her to take more time to identify the patient!